
Empiric treatment is not the broadest spectrum possible. Yes, they will put someone on Augmentin for a human bite, but that’s very different from putting someone on IV vancomycin or meropenem. The augmentin will probably cover anything in that bite, but if the culture comes back showing resistance, then you switch to something else.
- 5 Posts
- 231 Comments
Joined 9 months ago
Cake day: January 13th, 2024
You are not logged in. If you use a Fediverse account that is able to follow users, you can follow this user.
I’ve been in clinical rotations and my attending physicians have been very clear about antibiotic use and there is a lot of clinical evidence and guidance for minimizing broad spectrum use.
We like to use the narrowest spectrum antibiotics possible to limit side effects and breeding resistance. Also, the really broad spectrum ones are expensive.
Not even a sip for me. I was offered small amounts of champagne or wine at special occasions, but I never drank any because I could smell the alcohol on it and didn’t want to.
I’ve just always been some variant of the “mom friend” and after I turned 21, I was still the DD most of the time.
Nope. The first time I drank any alcohol ever was on my 21st birthday. My Dad made me a gin and tonic with Bombay Sapphire, and that set the standard for the kind of alcohol I will drink. It’s a good thing I’m a lightweight because I only drink the expensive stuff. (The cheap crap burns too much.)
I’ve tried to drink coffee a couple times. I never was successful at it. My body just hates something in coffee and it just comes right back up before even hitting my stomach. So, I guess it’s gone down my esophagus, but never further than that.
I end up going to the ER way more than I want to. It’s really annoying; if you walk into an urgent care or a regular doctor’s office (besides my regular care providers, they’re used to me now) and say you think you have a kidney infection or other kidney problems and you just need antibiotics, they just go “NOPE” and yeet you out the door to go to the ER. So far, I have been successful in preventing them from calling an ambulance for me.
Never have I ever drank alcohol illegally or underage.

 4·4 days ago
4·4 days agoAs an absurdly fervent Tolkien fan, people bringing up the Eagles spikes my blood pressure in a way that cannot be good in the long run.
 111·7 days ago
111·7 days agoMy original idea was for the AI companies to shell out for building new nuclear plants, but bringing an old one back online is a step in the right direction. I don’t think the current “AI” projects are actually worth the resources they consume, but if they’re going to exist, their creators should be shelling out for non-fossil fuel options to power them.
This is exactly what I’ve been advocating for. Nuclear power, especially if they lift the restrictions on fuel recycling, is the cleanest option we have besides solar and wind, and it’s a technology that is fully developed and available now. Nuclear power is heavily regulated and is very safe these days, and is not reliant on rare earth metals like many solar panels still are.
It takes years for a donor’s remaining liver to grow back, and the recipient is unlikely to grow out more of the donated liver depending on comorbidities and severity of illness.

I have done CPR on people before, and it is astonishingly brutal. To do it correctly, you have to cave their sternum in to be able to apply enough pressure to the heart to actually move blood around. For “Out of Hospital Cardiac Arrest” patients that receive bystander CPR, the survival to discharge is around 10%, give or take. The most common outcome of CPR (if it is successful and you get a pulse back) is days to weeks of dying slowly and painfully in the ICU. The older someone is, or the more health problems they have, the much lower the chance of recovery is.
CPR is absolutely reasonable for a younger person that stands a good chance of walking out of the hospital at the end of it, but 90 pound 90-year-old is extremely unlikely to survive in a meaningful way. It is very reasonable to request to not be put through that massive amount of suffering for a very low chance of any meaningful benefit.
There’s also degrees of DNR. There’s separate options for CPR, intubation, supportive care, active treatment, palliative care, etc. It’s a lot more nuanced than CPR yes/no in most situations.

The one my husband gave me is Nenya without the stones. It’s just the 6 petaled flower in white gold.

I got my husband an engagement watch. It’s an analog watch with a 24 hour dial, and it was very hard to find. He was delighted (especially since the ring he was getting made for me was delayed by about 4 months because of Covid)
 8·25 days ago
8·25 days agoThis is the mindset I have to keep myself in while working in medicine. I can’t save every patient. Some of them will die in my care, but that won’t stop me from trying to help the next one.
 2·27 days ago
2·27 days ago(To be fair, I did manage to run Half Life: Alyx and Beat Saber on a 1060)
 0·28 days ago
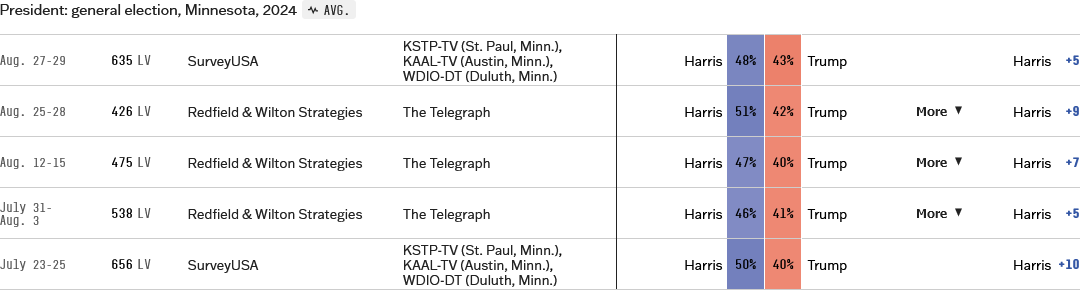
0·28 days agoWhat in the hell are you talking about? Kamala’s lead is variable, but substantial.





{kind=link}
Correct. I’m a third year medical student on my clinical rotations right now, and I worked in the medical field for 4 years before starting med school.